If you prefer videos, watch the youtube video where we cover what consent is, how to obtain consent from children including Gillick competence and consenting vulnerable adults with the Mental Capacity Act of 2005.
Today’s blog is all about obtaining valid consent which is the third GDC principle. We’ll be covering a quick history on English tort law cases to do with negligence and then we’ll talk about what valid consent actually is, followed by consenting children under 16 and then we’ll finish by talking about consenting vulnerable adults who don’t have the capacity to consent for themselves.
Bolam/Montgomery
So I’m not gonna bore you guys for too long with the history of it all, but just a bit of background on case law to do with negligence. In 1957, Mr Bolam, a man undergoing electro-convulsive therapy at a mental health institution wasn’t informed of what the treatment involved and wasn’t given muscle relaxants while being treated and so he suffered serious injuries. He ended up suing the hospital management committee and because of it, the Bolam test became a part of the law and it basically stated that if a medical professional reaches the standards of a responsible body of medical opinion, than that medical professionals actions would not be negligent.
In 2015, the case law of Montgomery v Lanarkshire Health Board disregarded and replaced the Bolam test with a greater test in negligence by stating that “The doctor is under a duty to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and their reasonable alternatives. “Material risks” here includes what a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.
Valid Consent
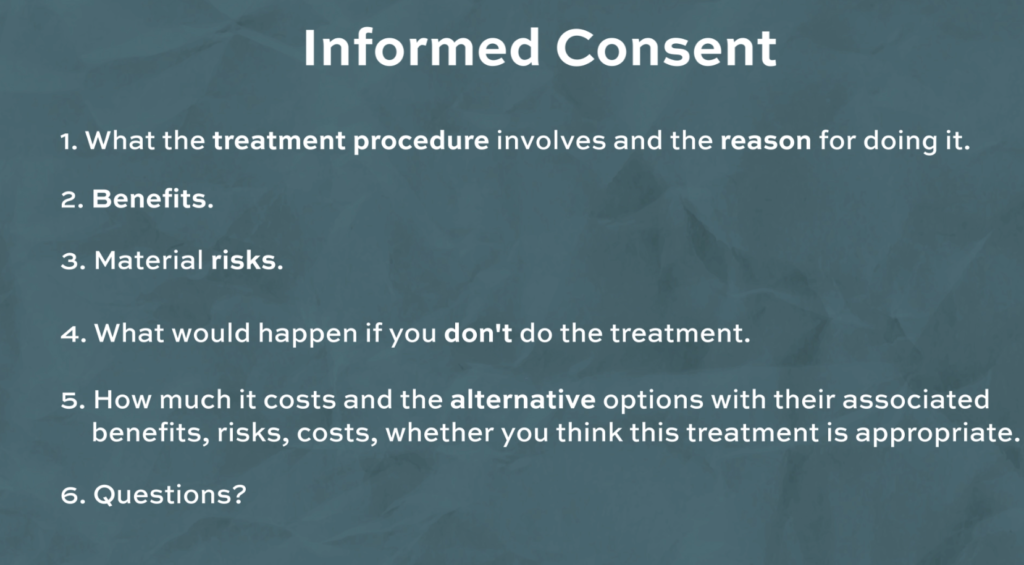
Okay so for consent to be valid it needs to be voluntary, informed and obtained by the correct authoriser who must have capacity. Without valid consent, you’d be assaulting the patient so that’s only more reason to make sure you to properly understand what consent encompasses. Voluntary means that the dentist can’t influence the patient to make a decision by pressuring them into doing what they want. Informed consent, as defined by the GDC, is achieved if the patient has received enough information to make a decision and we’ll go through what this means. There are 6 things which should be discussed with the patient. The first is what the treatment procedure involves and the reason for doing it. Then we need to inform them of the benefits and material risks of the treatment. You’d need to tell them what would happen if you don’t do the treatment. How much it costs and the alternative options with their associated benefits, risks, costs and whether you think this treatment is appropriate. Finally, you should also check to see if they have any questions regarding what you’ve just discussed.
And finally capacity refers to if the patient can communicate back to you what you have explained to them which displays proper understanding. The information needs to be retained and evaluated so that the benefits and risks can be weighed up so that a decision can be made. Its important to note that consent is an ongoing process between the dentist and the patient and they have the right to withdraw consent at any point including during the procedure.
Types of Consent
There are 3 ways to give consent and the first type is non-verbal (or implied) and an example of this is if the patient sits in the chair than it’s implied that they accept for you to carry out an initial examination. The second type of consent is verbal and this is needed for treatments like fillings and scales and the last type is written consent which is needed for treatments which have bigger risks attached to the treatment, like going under a general anaesthetic or needing a surgical extraction.
Consenting Children
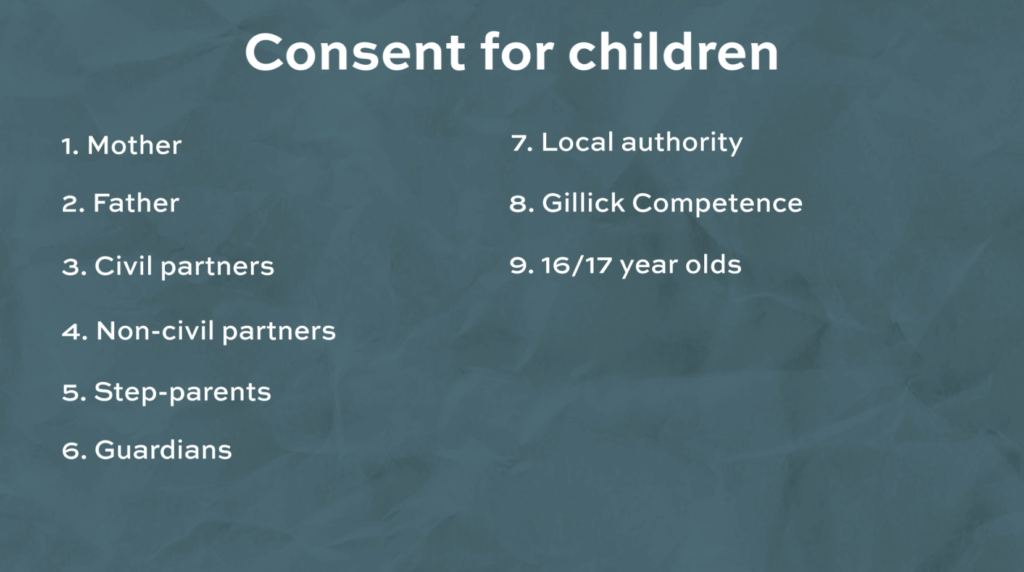
Now we’ll move on to talking about who can consent for children under 16. There are 9 groups we’ll mention here and the first is a child’s Mother. The second is a child’s father if he was on the birth certificate but it used to be a bit different if the child was born before December 1st 2003. The third is civil partners, they need to have been civil partners at the time of conception which is either donor insemination or fertility treatment. Next is consent for Non-civil partners and this is achieved by the 2nd parent applying for a parental responsibility agreement after becoming a civil partnership or alternatively they would both have to jointly register at birth. The 5th and 6th are for step parents and guardians who need a parental responsibility agreement from the the biological parents or a court order. The 7th is if the local authority has consent which can be joint with the parents if there’s a court order but if the child was under the care of the local authority voluntarily, than the parents would still be responsible.
The next is to to do with Gillick competence which states that a child who is younger than 16 can consent for themselves without the presence or knowledge of their parents if they are competent and have capacity so they fully understand the treatment in such a way that they can communicate it back to you and can weigh up the benefits and risks and retain that information. It’s important to note that while a child can consent for treatment to happen, if they refuse treatment and the parent consents to the treatment, the child’s decision would be overruled. It’s also important to note that a child might be able to consent for certain treatments but not for others because while they might be able to communicate, understand, retain and evaluate for a fissure sealant they might not be able to communicate, understand, retain and evaluate the options for a maxillofacial surgical procedure. The last group is younger children who are 16 or 17 year olds and this group can consent for themselves and can’t be overruled by their parents but in certain circumstances a court order might be used and this can overrule the child’s decision.
Vulnerable Adults
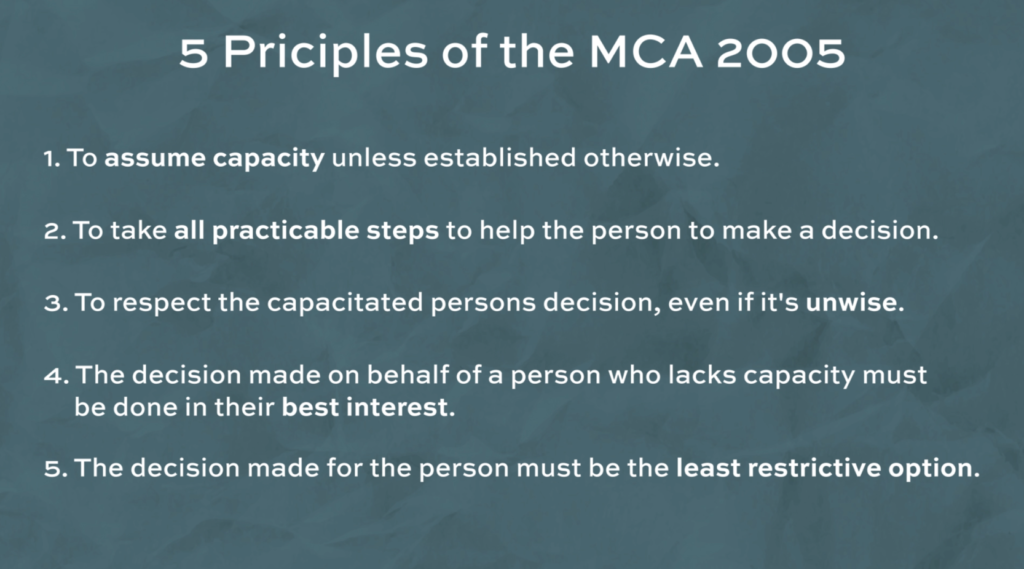
Finally I’ll be speaking about vulnerable adults and the way you test this is with 2 questions: 1. Does the patient have an impairment of, or a disturbance affecting the functioning of their mind? and 2. Does that impairment or disturbance mean that the person is unable to make a specific decision when they need to? You also need to constantly re-assess capacity each time a decision needs to be made and this is especially for patients who have fluctuating capacity. If you think that a patients will regain capacity then if possible, you should delay the decision making process . There are 5 main principles mentioned in the MCA of 2005 which have to be considered, and these are: 1. To assume capacity unless established otherwise. 2. To take all practicable steps to help the person to make a decision. 3. To respect the capacitated persons decision, even if it’s unwise. 4. The decision made on behalf of a person who lacks capacity must be done in their best interest. And finally 5. The decision made for the person must be the least restrictive option.
When an adult needs to make a decision but doesn’t have capacity, you need to find out if they have made any advanced decisions to refuse treatment, if they have a lasting power of attorney or if the court of protection are involved in anyway. If none of the above applies to a particular patient then you need to act in the best interest of the patient.
An advanced decision, sometimes known as a living will, allows someone who is both over 18 and had capacity at the time of making the decision to refuse certain treatments in the future.
A lasting power of attorney is a legal document which is given to a close family member or friend on behalf of the patient who might be expecting to lose capacity in the future. There are 2 types of LPA’s and one type is for personal welfare and the other is financial and the one you need to look out for is the personal welfare LPA. Again the patient needs to be over 18 and have capacity at the time they appoint someone to be their attorney and they must be registered with the office of public guardian.
So if you’ve checked and it turns out the patient doesn’t have an ADRT or a LPA than you need to act in the best interest of the patient. You need to try and involve the patient and their family as much as possible and consider the patients past wishes and if there is significant risks associated with carrying out the treatment you’ll need to request an IMCA, an independent mental capacity advocate who can make sure the treatment is worth doing by weighing up the benefits and risks for the patient and making sure their rights are upheld. Usually these IMCAs are quite good at getting an in-depth understanding and could speak to loads of different medical professionals from the GDP to the patients GP to any specialists involved and even sometimes the anaesthetist.
Check out our other content
If you’re interested, feel free to check out our other Blogs, our Instagram page, or our YouTube channel for more.